
Chylothorax in Dogs - Case Study
Clyde is a 5-year-old 65kg Bull Mastiff who stole all our hearts!
He was seen at his referring veterinarian after a week-long history of lethargy, tachypnoea and inappetence. Thoracic radiographs were performed and showed a fluid/soft tissue opacity that obscured the majority of the lung fields and cardiac silhouette. Thoracocentesis was performed and one litre of chyle-like fluid was removed.
The removed fluid was submitted for evaluation and revealed a lymphocyte-rich effusion with triglyceride levels higher than in serum. Clyde was referred to the Adelaide Veterinary Specialist and Referral Centre, Medicine Department for investigation.

Clyde, the Bull Mastiff
Differential diagnoses for chylothorax included:
- Pericarditis/Cardiac disease
- Intrathoracic mass e.g. thymoma, or cranial mediastinal neoplasia
- Thoracic duct occlusion
- Thromboembolic disease
- Inflammatory disease
- Idiopathic chylothorax.
A diagnostic plan included thoracic ultrasound and echocardiogram with a view to performing a CT scan if there was no pathology evident on the ultrasound examination. Right sided congestive heart failure can contribute to increased venous return and hence pleural effusion. A small degree of tricuspid valve disease was noted on the ultrasound examination but not considered significant particularly in light of there being supporting clinical signs.
No specific causes could be found on CT scan and therefore an idiopathic diagnosis was made. Ultrasound guided thoracocentesis was performed from the right thorax and additional chyle removed. Clyde was monitored over the following 12 months and after initial resolution developed recurrent episodes of coughing and dyspnoea with an acute life-threatening episode of chylothorax where four litres of chyle was removed.

The chyle fluid removed.
Emergency thoracocentesis was performed on the patient in sternal recumbency. Using local anaesthetic and a small skin cut down, large 14 G over the needle catheters were inserted dorsal to the costochondral junction at the 8th intercostal space. Fluid was then removed using extension tubing attached to a 3-way stop cock and 50ml syringe.
If back pressure was encountered gently tilting him to the dependant side and manipulating the catheters trajectory into the chest allowed for maximal flow. Medical management including low-fat dietary modification helps and patients occasionally resolve spontaneously but idiopathic forms often require thoracic duct ligation to stop the effusion. Chronic effusion has also been shown to increases the risk of fibrosing pleuritis which in itself causes dyspnoea, hence Clyde’s owners elected to proceed to surgery.
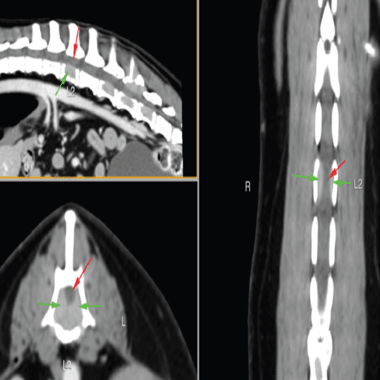
Pre-operative CT lymphangiography can help visualize the various branches of the thoracic duct. This may be performed by injecting Iohexol contrast agent into either the popliteal, mesenteric lymph nodes or an iodine contrast agent subcutaneously around the anus. Intraoperative mesenteric lymphangiography and fluoroscopy has also been described. A practical technique and one used in this case involved diluted methylene blue injected into a lymphatic or intranodally. This is very helpful in identifying all branches of the thoracic duct helping to ensure complete ligation.
Clyde was positioned in left lateral recumbency and a right sided ninth intercostal thoracotomy performed after he was placed on a ventilator. A local block was carried out at the two ribs cranial and caudal to the thoracotomy using Bupivacaine. A further 200ml of chyle was suctioned and the chest lavaged with saline.
The pleura was thickened on its reflection at the mediastinum. The aorta, sympathetic chain and azygos vein were identified. A para costal incision was made and after exteriorising a loop of duodenum, an attempt at catheterisation of an efferent lymphatic for lymphangiography was performed. The lymphatics were very friable and after two attempts at catheterization this was abandoned.
A lymph node at the ileocolic mesentery was then injected with 0.5ml of methylene blue and then five minutes later. The thoracic duct and its associated branches could be now be clearly visualised in the right mediastinum. Three large ducts could be seen in the peri aortic tissue and three 10mm liga clips were applied. A 2cm incision was made dorsal to the aorta and a number of smaller ancillary branches were seen.

Thoracic duct ligation using a combination of Prolene and Liga clips after coloration of a mesenteric lymph node with methylene blue.
An encircling 2/0 Prolene ligature was passed through the mediastinum and used to ligate these en bloc. A right sided subtotal pericardectomy was performed by making a T-shaped incision ventral to the phrenic nerve and extending to the apex of the heart thereby removing a triangular area of thickened pericardium. The chest and abdomen were lavaged with copious amounts of warm saline and a chest drain placed.
Layered closure of the thoracotomy and para costal incision was performed. After surgery, Clyde was closely monitoring by a dedicated hospital team overnight, then spent a few days with our Emergency and Critical Care Team. Clyde has done extremely well post operatively and at three months has no further symptoms.

The chyle removed
Reference
Small Animal Surgery
5th Edition, Theresa Welch Fossum, 2018, CV Mosby Publishing):
Dr Bruce Meyers MMED Vet (Small Animal Surgery)
Adelaide Veterinary Specialist and Referral Centre
102 Magill Road Norwood, 5067 - Ph: (08) 8132 0533
Biography of Dr Bruce Meyers
Dr Meyers qualified as a veterinarian in 1993 and completed his Master’s Degree in Small Animal Surgery in 2008 at the University of Pretoria (Onderstepoort). Dr Meyers is registered as a Specialist Veterinary Surgeon with the South African Veterinary Council, and he established St Helier Veterinary Hospital and Specialist Centre in Durban, before he relocated to Adelaide in January 2022 with his wife, daughter and their three dachshunds. Bruce is a keen mountain biker, loves kite surfing, the ocean and spending time with his family.

You can read more of our specialist veterinary news and stories here.
For referring vets, please use our online referral form to submit a case enquiry.
You might also be interested in
Bone Cancer in Dogs | Cancer Treatment in Dogs Case Study
Read about bone cancer in dogs and cancer treatment in dogs. Meet Kimba who was diagnosed and treated by the Animal Referral & Emergency Network.

Auto-Immune Disease in Pets | Diagnosis & Treatment
Cranial Cruciate Ligament Rupture & Treatment
Rupture of the cranial cruciate ligament (CCL) is the most common cause of persistent hindlimb lameness in dogs. Read about cruciate ligament condition.
